
This Dr. Axe content is medically reviewed or fact checked to ensure factually accurate information.
With strict editorial sourcing guidelines, we only link to academic research institutions, reputable media sites and, when research is available, medically peer-reviewed studies. Note that the numbers in parentheses (1, 2, etc.) are clickable links to these studies.
The information in our articles is NOT intended to replace a one-on-one relationship with a qualified health care professional and is not intended as medical advice.
This article is based on scientific evidence, written by experts and fact checked by our trained editorial staff. Note that the numbers in parentheses (1, 2, etc.) are clickable links to medically peer-reviewed studies.
Our team includes licensed nutritionists and dietitians, certified health education specialists, as well as certified strength and conditioning specialists, personal trainers and corrective exercise specialists. Our team aims to be not only thorough with its research, but also objective and unbiased.
The information in our articles is NOT intended to replace a one-on-one relationship with a qualified health care professional and is not intended as medical advice.
6 Best Steps to Care for the Dying
November 23, 2018

The goal of comfort care, another way to describe medical care for the dying or seriously ill, is to help honor the wishes of the patient. Caring for the dying during the end-of-life stage commonly involves a combination of medical, social, emotional, spiritual and practical support. Doctors, nurses, social workers, nutritionists, aids and spiritual advisers can all play a role in offering quality care for the dying.
As an article published in the British Journal of Medicine puts it, “Ensuring a good death for all is a major challenge not only for healthcare professionals but also for society.” (1) Fortunately, evidence-based guidelines now exist to help with care for the dying, including guidelines for symptom and pain control, emotional support and bereavement care.
It’s possible for end of life care (or hospice care or palliative care) to be offered in various settings, such as at home, in a hospital where treatment can be given for as long as possible, at nursing homes, outpatient palliative care clinics or in a hospice center. No matter the location, the goal is to honor each individual’s wishes, including where they want to be and who they want to be present while they are nearing death, including family or friends, for example.
What Is Comfort Care?
According to the National Institute of Aging, comfort care is considered “care that helps or soothes a person who is dying.” It is thought of as an essential part of medical care at the end of life because its benefits include: (2)
- Preventing or relieving suffering
- Helping to improve quality of life as much as possible
- Respecting the dying person’s wishes while ensuring a peaceful death
- Reducing distress experienced by the dying individual’s family members and friends
Care for the dying focuses on four general types of needs that individuals who are nearing death experience: physical comfort, mental and emotional needs, spiritual issues and practical tasks. One of the most important aspects of comfort care is allowing patients to choose where they stay during the end of their life. (3) Surveys show that most individuals with serious, advanced illnesses preferred to die at home and receive a more conservative pattern of end-of-life care rather than dying in hospitals.
What types of patients receive comfort care? Older adults and anyone with a terminal or serious illness — such as heart disease or heart failure, chronic obstructive pulmonary disease (COPD), cancer, dementia, Parkinson’s disease, lung diseases, kidney or liver failure, HIV/AIDS, ALS, and many others — may choose to receive comfort care. Many of these conditions are the top causes of death worldwide, so you can see why comfort care is in such high demand.
There are several different types of comfort care, including hospice or palliative care, which are all considered “multi-disciplinary” approaches. They tend to combine treatment options that often include: pain medication or management, emotional support, physical or occupational therapy and counseling on practical problems such as finances, transportation, housing and other resources.
How do you know if someone is ready for comfort care? What are signs to look for at the end of life? In order to provide quality care, it’s important for healthcare workers to recognize the key signs and symptoms of dying, and to openly discuss this with patients and their caregivers so everyone knows what to expect. Those who are nearing the end of their life tend to experience symptoms including: (4)
- Coolness in the hands, arms, feet and legs
- Changes in skin color, including paleness and purpleness
- Confusion
- Decreased urine output
- Hallucinations
- Forgetfulness and dementia, including forgetting family members and friends
- Trouble breathing, congestion and gurgling in the chest
- Trouble speaking normally, clearly and truthfully
- Chronic fatigue and spending extra time sleeping
- Incontinence (losing control of urinary/bowel functions)
- Making repetitive movements
- Loss of appetite
- Social withdrawal and depression
- Restlessness
- Teary, glassy eyes
How long can someone remain in the active stage of dying? It depends on the cause of death, since each person’s experience is unique. End of life symptoms may last for about three to six months, but sometimes they occur for longer or shorter durations. It ultimately depends on the extent of symptoms management, treatments and also the person’s outlook and medical history.
Comfort Care vs. End of Life Care vs. Hospice vs. Palliative Care
- Is there a difference between comfort care, end of life care and hospice? Comfort care and end-of-life care are mostly used interchangeably and describe the same thing: care for the dying, or care for patients at the end of their life. These are both similar to hospice, although hospice tends to be for a shorter duration of time.
- Hospice care usually begins after treatment of a serious disease is stopped, when is someone is expected to pass away shortly after, usually within 6 months or so. Compared to hospice, comfort care can last longer and be ongoing. (5)
- What is palliative care? Palliative care is treatment for seriously ill patients, which can include a combination of curative treatments to help extend lifespan and also symptom management to reduce discomfort. When receiving palliative care, a patient doesn’t need to stop treatments that might cure a serious illness; they can continue treatment and also receive care for other physical and emotional symptoms. Palliative care can begin as soon as someone is diagnosed with a serious illness and might include physical therapy, occupational therapy, nutritional therapy, pain management and other integrative therapies.
- A patient may receive palliative care throughout treatment, during follow-up and at the end of life. (6) The main difference between palliative care and hospice is that in hospice, attempts to cure the person’s illness are stopped.
- Depending on how an individual’s disease progresses, palliative care may transition to end-of-life care or hospice care, usually if the doctor believes the person is likely to pass away in the near future. Depending on the patient’s preferences, hospice can and end-of-life care can be provided at home, in a nursing home, in an assisted living facility or an inpatient hospital. (7)
The modern care for the dying, or hospice/palliative care movements, were established in response to the poor quality of care offered to many dying patients. To ensure that as many patients as possible die peacefully, diagnosing dying is now considered an important clinical skill among healthcare workers. More nurses, aids and workers are receiving formal training to care for the dying with a variety of treatment approaches.
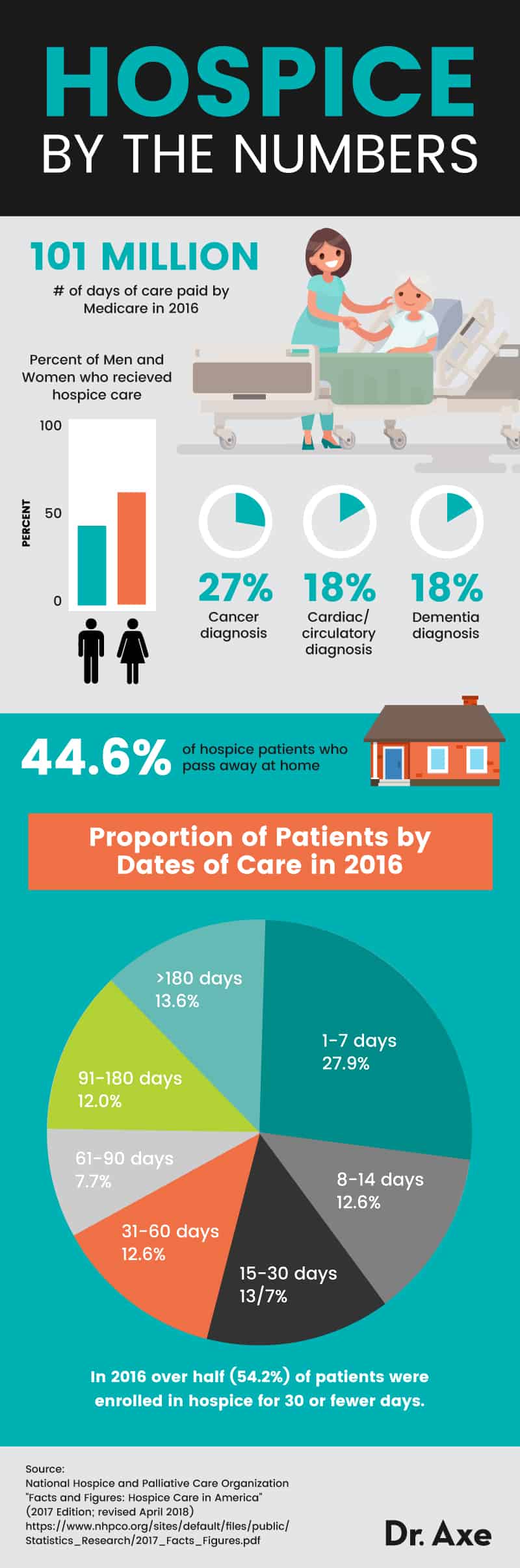
How are all of these services usually paid for? Care for the dying or seriously ill can be paid for through a combination of Medicare, Medicaid, private insurance policies or the Department of Veterans Affairs for veterans.
6 Best Steps to Care for the Dying
1. Manage Pain and Reduce Discomfort
Pain at the end of life can be due to various health issues, such as those that cause symptoms like: trouble breathing, digestive issues like loss of appetite or nausea, skin irritation or rashes, temperature sensitivity, fatigue, weakness and others. Pain can also increase irritability, interfere with sleep and appetite and make it difficult to spend meaningful time with loved ones when it matters most.
What are some comfort care measures that can be used to reduce pain?
When it comes to end-of-life care, pain management may be different than during other life stages. This is for a variety of reasons, including less concern about possible long-term problems associated with pain medications, drug dependence or abuse. This is why care-for-the-dying experts recommend using pain medications at dosages that help bring relief, and this includes even strong medications such as morphine. There is not much evidence that pain medications shorten life span, but there is evidence that they provide much needed comfort to those who are close to dying.
Non-essential drugs should also be discontinued in order to reduce any unnecessary side effects. Drugs that do need to be continued may include opioids, anxiolytics and antiemetics. They are often switched to subcutaneous administration or administered continuously via infusion if appropriate.
Other than pain medications, caregivers may ease discomfort through intravenous fluids, touch or gentle massage, music, therapy, psychological support, or in some cases use of some herbs/supplements.
2. Ease Symptoms Like Trouble Breathing, Digestive Issues & Skin Irritation
Near the end of life, many patients experience trouble breathing and other symptoms like loss of appetite, fatigue and skin-related issues.
Some ways to help improve breathing include: raising the head of the bed, opening a window to allow fresh air in, using a humidifier if the air in the room is dry and using a circulating fan. Morphine or other pain medications are also sometimes used to decrease the sense of breathlessness. Caregivers can also help reduce congestion by gently turning the patient’s head to the side to drain secretions, wiping their mouth with a moist cloth and diffusing essential oils like peppermint.
If digestive issues are causing discomfort, patients can benefit from meeting with a dietician or nutrition counselor for guidance about foods to emphasize and avoid. However, at the end of life, it’s best not to force someone to eat or drink if they don’t want to, since this increases discomfort and irritability. It’s best to offer water, small chips of ice or frozen juice chips, soups, yogurt or other easy-to-eat and refreshing foods. If incontinence becomes an issue, a nurse or caregiver can help keep the patient comfortable by changing their clothes often and keeping them clean.
It’s important to take extra care of fragile, aged skin towards the end of life. A cool, moist cloth can be used to gently cleanse skin.

3. Create a Comfortable Environment (Temperature and Lighting)
Because many people tend to feel cool as they near death, it’s helpful to keep them warm with comfortable, soft blankets and a temperature-controlled room. In the case that a fever develops, keeping the room cool and applying a cool cloth to their head is useful.
If the patient wants to spend extra time sleeping or closing their eyes, those around them can help make them feel comfortable by also staying quiet, speaking in a normal to soft voice, gently holding their hand and keeping the lighting in the room low or soft. As long as the patient is okay with it, lightly massage their forehead, read to them, diffuse essential oils for anxiety (such as lavender and chamomile) and/or play soothing music to help make the environment seem calmer.
4. Deal with Emotional Pain and Suffering
An important aspect of care for the dying is emotional and social support. A team of mental health providers, such as a therapists or counselors, can help with handling stress, anxiety and uncertainty during this difficult time. Therapy, family meeting and support groups are all useful for reducing fear, hopelessness or depression towards the end of life.
5. Address Spiritual Needs
Many people nearing the end of their life will seek spiritual help to find comfort, meaning and faith. It’s common for spiritual advisors to visit patients in hospice, at home or at a hospital in order to help them find acceptance and peace, sometimes through healing prayer. This can be beneficial not only for the patient who is dying, but also for their caregivers and family who are grieving.
6. Assign Everyday Tasks to a Supported Caregiver
Studies show that it’s very important for caregivers and families to receive clear information and answers to questions while a loved one is dying. Healthcare teams are often trained to offer emotional support, respect and compassion and a willingness to answer family questions so expectations are clear.
If you’re a caregiver to a parent, spouse or another person nearing death, discuss end-of-life care options with the dying person, find out their preferences and make sure you are clear on your rights and duties as the caregiver.
Things to discuss include: whether or not you will use life-extending treatments, how long he or she has left to live and the preferred setting for care. Caregivers are often referred to counselors to discuss everyday concerns like finances, insurance, job-related problems and legal issues. It can be helpful to find a care team that can explain complex medical forms, help provide financial counseling and arrange resources for transportation or housing if needed. Even though it can be very difficult to discuss final arrangements, it’s often comforting to a patient if they can share what’s important to them and their preferences.
Can you still hear when your dying? Some patients might withdraw and be unresponsive, but in most cases hearing remains, which means that caregivers can speak in a normal voice, identify themselves, hold their love one’s hands and express how they feel.
Know that it’s normal for caregivers and grieving family/friends to experience a rush of different emotions when someone close to them dies. Some people describe this as the stages of grief, or stages of death/dying. What are the five stages of death and dying? The five stages include: denial, anger, bargaining, depression and acceptance. All of these can occur while someone learns to cope with loss and their feelings. (7)
Final Thoughts
- Another name to describe care for the drying is comfort care, defined as multi-disciplinary care that helps or soothes a person who is dying.
- Care for the dying is thought of as an essential part of medical care at the end of life because it includes benefits like: preventing or relieving suffering, helping to improve quality of life, respecting the dying person’s wishes, ensuring a peaceful death and reducing distress for the dying individual’s family members and friends.
- Comfort care and end-of-life care are mostly used interchangeably to describe care for patients at the end of life. Hospice tends to be for a shorter duration of time, within 6 months of expected death. Palliative care can start once a diagnosis is made and continue for months until it transitions to hospice or comfort care.
- The six best steps to care for the dying include: managing pain/reducing discomfort, easing symptoms like breathing trouble and digestive issues, creating a comfortable environment, dealing with emotional pain, addressing spiritual needs and assigning tasks to a chosen caregiver.
