This Dr. Axe content is medically reviewed or fact checked to ensure factually accurate information.
With strict editorial sourcing guidelines, we only link to academic research institutions, reputable media sites and, when research is available, medically peer-reviewed studies. Note that the numbers in parentheses (1, 2, etc.) are clickable links to these studies.
The information in our articles is NOT intended to replace a one-on-one relationship with a qualified health care professional and is not intended as medical advice.
This article is based on scientific evidence, written by experts and fact checked by our trained editorial staff. Note that the numbers in parentheses (1, 2, etc.) are clickable links to medically peer-reviewed studies.
Our team includes licensed nutritionists and dietitians, certified health education specialists, as well as certified strength and conditioning specialists, personal trainers and corrective exercise specialists. Our team aims to be not only thorough with its research, but also objective and unbiased.
The information in our articles is NOT intended to replace a one-on-one relationship with a qualified health care professional and is not intended as medical advice.
How to Treat Postpartum Depression, Which Affects Both Mom & Baby
April 10, 2016

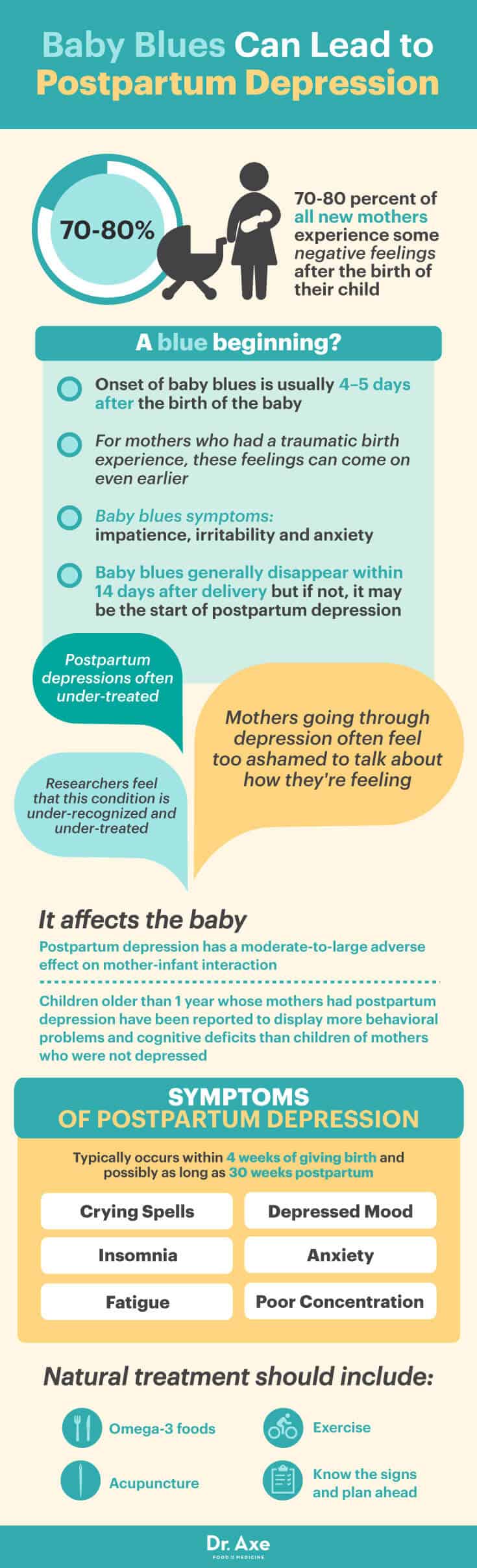
Did you know that 70–80 percent of all new mothers experience some negative feelings after the birth of their child? It’s common for women to experience severe mood swings after giving birth, which are known as baby blues. But when this sense of sadness doesn’t go away, it may be the start of postpartum depression.
Mothers going through depression often feel too ashamed to talk about how they’re feeling, and researchers feel that this condition is both under-recognized and under-treated. Mothers don’t feel like they’re being “good mothers” and often feel guilty about not wanting to take care of their newborn.
For most women, these feelings of inadequacy and sadness go away naturally, but for some this can turn into lasting depression, which can hinder the relationship between the mother and child. In fact, researchers have reported that postpartum depression has a moderate-to-large adverse effect on mother-infant interaction. Children older than 1 year whose mothers had postpartum depression have been reported to display more behavioral problems and cognitive deficits than children of mothers who were not depressed. For this reason, it’s important to understand the symptoms of ongoing postpartum depression and take these mood swings and phases seriously. (1)
The time following the birth of a child is one of intense physiologic and psychological change for a new mother. For mothers who are experiencing these changes, talking about their emotions and challenges is one of the best ways to cope with postpartum depression. It’s crucial to identify and treat women with postpartum depression as early as possible, but the problem often continues due to lack of identification. Identifying women at risk and providing early treatment interventions are the first steps in dealing with this devastating illness. And the good news is that there are natural and safe ways to reduce the symptoms of depression and relieve stress, helping new moms to feel like themselves again as they embark on this new and sometimes scary journey.
Symptoms of Postpartum Depression
While roughly three-quarters of all new mothers experience baby blues 4–5 days after the birth of the baby, for mothers who had a traumatic birth experience, these feelings can come on even earlier. Mothers with baby blues often experience the symptoms of postpartum depression, such as impatience, irritability and anxiety. These feelings generally disappear within 14 days after delivery.
But when these mood swings continue past a 2-week period, it may be a sign that the woman is going through postpartum depression. According to the American Journal of Obstetrics and Gynecology, postpartum depression affects up to 15 percent of mothers. (2)
Postpartum depression typically occurs within 4 weeks of giving birth and possibly as long as 30 weeks postpartum. Symptoms of postpartum depression include:
- Crying spells
- Insomnia
- Depressed mood
- Fatigue
- Anxiety
- Poor concentration
The diagnostic criteria for a Major Depressive Episode is no different in the postpartum period compared to other episodes of depression. To be considered depression, the patient has experienced at least two weeks of persistent low mood, as well as four of the following: increased or decreased appetite, sleep disturbance, psychomotor agitation or retardation, feeling always tired, feelings of worthlessness, low concentration and thoughts of suicide.
A mother may be diagnosed with postpartum depression if the symptoms begin within the first 4 weeks of delivery, but some studies suggest that depressive episodes are significantly more common in women in the first three months after delivery. In addition to this, an increased vulnerability to psychiatric illness or mental disorders may persist for a year or more after giving birth. (3)
Causes of Postpartum Depression
Studies have looked at possible causes of postpartum depression, including hormonal fluctuation, biological vulnerability and psychosocial stressors, but the specific cause remains unclear.
Many psychological stressors may have an impact on the development of postpartum depression. Recent studies conclude that the majority of factors are largely social in nature. According to the Journal of Clinical Psychiatry, the greatest risk for developing depression after pregnancy is in women with a history of depression or other affective illnesses, and in those who have experienced depression during past pregnancies. Postpartum depression causes significant suffering in women at a time when personal and societal ideas of motherhood are feelings of joy.
When a new mother doesn’t feel gratification in her new role, and she doesn’t feel a connection with her infant or have the ability to carry out the often overwhelming task of caring for a new baby, this often leads to a sense of isolation, guilt, helplessness and hopelessness that characterize a depressed state. Because postpartum depression exists as part of the spectrum of major depression, researchers suggest that women with significant risk factors should be followed closely in the postpartum period.
It is also possible that no biological factors are specific to the postpartum period, but that the process of pregnancy and childbirth represents such a stressful life event that vulnerable women experience the onset of a depressive episode. (4)
Research published in the Journal of Obstetric, Gynecologic and Neonatal Nursing suggests that caregivers use a checklist to identify women at risk for developing postpartum depression. The following predictors for postpartum depression were pinpointed:
- Prenatal depression — Depression during pregnancy that occurred in any trimester.
- Child care stress — Stress related to the care of a newborn, especially with infants who may be fussy, irritable and difficult to console, or who are struggling with health troubles.
- Support — A real or perceived lack of support, including social support, emotional support and help at home.
- Life stress — Stressful life events that occur during both pregnancy and the postpartum period.
- Prenatal anxiety — A feeling of uneasiness about an obscure, nonspecific threat.
- Marital dissatisfaction — The level of happiness and satisfaction with a partner, including feelings about her marriage and relationship.
- History of previous depression — Women with a history of major depression. (5)
A review published by the International Journal of Women’s Health found that women with postpartum depression are at a higher risk for smoking, alcohol or illicit substance abuse, and are more likely than non-depressed mothers to experience current or recent physical, emotional or sexual abuse. Thoughts of self-inflicted injury or suicide are also signs of postpartum depression.
A recent World Health Organization report on women’s health identified self-inflicted injury as the second leading cause of maternal mortality in high-income countries, and suicide remains an important cause of maternal deaths in moderate and low-income countries. Intrusive thoughts of accidental or intentional harm to the baby are common in the early stages of new motherhood, but these thoughts are more frequent and distressing in women with postpartum depression. (6)
How Does Postpartum Depression Affect the Infant?
Because depression has significant negative effects on a mother’s ability to interact appropriately with her child, there is an adverse impact of postpartum depression on the infant. Depressed women have been found to have poorer responsiveness to infant cues and more negative, hostile or disengaged parenting behaviors. When the mother-infant interaction is disrupted in this way, studies have found that there is lower cognitive functioning and adverse emotional development in the child, which appears to be universal across cultures and economic statuses. (7)
Mothers with postpartum depression also increases the risk of experiencing issues with infant feeding. Research shows that depressed mothers have difficulty breastfeeding, with shorter breastfeeding sessions that can impact the baby’s nutrition. There is also beginning evidence to suggest that depressed women may be less likely to initiate breastfeeding and stick it to. (8)
A study conducted at the Research Institute for Children’s and Women’s Health in Vancouver found that chronic depression in mothers places children at a higher risk for behavioral problems and psychological issues, such as anxiety, disruptive and affective disorders. But remission of depression in mothers was associated with a reduction or remission in the children’s psychiatric diagnoses. (9)
3 Conventional Treatments for Postpartum Depression
Early detection and treatment of depression after and during pregnancy is important because of the many adverse outcomes, including infant care and development. Experts have recommended screening for postpartum depression at the first postnatal obstetrical visit, which is typically 4–6 weeks after delivery. As a screening tool, many healthcare practitioners use a 10-item self-report that emphasizes emotional and functional factors.
1. Psychotherapy
Common forms of psychotherapy include interpersonal therapy and short-term cognitive-behavioral therapy. Family physicians are key players in the detection and treatment of postpartum depression; this is because new mothers have a tendency to negate their feelings as something other than a treatable psychiatric illness. Depressed mothers also report that they don’t receive the social support that they desire in this time of need. This lack of perceived support occurs in women’s relationships with their parents, relatives and friends, but it most pronounced in their relationships with their partners.
Interpersonal psychotherapy is a short-term, limited focus treatment that targets the specific interpersonal disruptions experienced by women in the postpartum period. Plus, a recent systematic review found that patients with major depressive disorder in primary care actually prefer psychotherapy over antidepressant medication for treatment, especially women with postpartum depression.
One study reported that 31 percent of breastfeeding women with postpartum depression declined antidepressant medication because they were breastfeeding; these women are better suited for psychotherapy as a conventional treatment option. Several studies show the positive results of psychotherapy, both in an individualized setting and in a group format. (10)
2. Antidepressant Medication
Postpartum depression demands the same pharmacologic treatment as major depression does, with similar doses as those given to patients with depression that isn’t associated with pregnancy. Selective serotonin reuptake inhibitors (SSRIs) are usually the first-choice medicines for women with postpartum depression. They can ease the symptoms of moderate-to-severe depression by affecting blocking the reabsorption of the neurotransmitter serotonin in the brain. Changing the balance of serotonin may help brain cells send and receive chemical messages, which boosts mood.
Tricyclic antidepressants are also commonly prescribed. This type of medication eases depression by affecting naturally occurring chemical messengers (neurotransmitters), which are used to communicate between brain cells.
Researchers suggest that mothers should continue medication for 6–12 months postpartum to ensure a complete recovery; however, there are concerns of breastfeeding mothers about exposure of the infant to the antidepressant medication. Infants are especially vulnerable to potential drug effects due to their immature hepatic and renal systems, immature blood-brain barriers and developing neurological systems. There are also concerns that treatment with antidepressant medication may result in metabolic changes in the postpartum period, and may effect the mother’s ability to care for a new baby.
A 2003 study published by the Journal of the American Board of Family Practice suggests that of the more frequently studied antidepressant drugs in breastfeeding women, paroxetine, sertraline and nortriptyline have not been found to have adverse effects on infants. Fluoxetine, however, should be avoided in breastfeeding women. (11)
3. Hormone Therapy
Because there is a dramatic drop in maternal levels of estrogen and progesterone at the time of delivery, this shift may contribute to the onset of postpartum depression in some women and hormone therapy may be beneficial. Estrogen has been used as a treatment of postpartum depression and some studies have showed promising results.
However, estrogen therapy should not be used in women with an increased risk of thromboembolism, and estrogen therapy can interfere with lactation, cause endometrial hyperplasia and elevate the risk of endometrial cancer. (12)
Natural Treatment for Postpartum Depression
1. Omega-3 Fatty Acids
According to researchers at The University of Kansas Medical Center, there is a growing body of clinical evidence that suggests that low dietary intake or tissue levels of omega-3 fatty acids are associated with postpartum depression. Omega-3 benefits are known to include relieving depression and feelings of anxiety. Low tissue levels of DHA are reported in patients with postpartum depression and the physiological demands of pregnancy and lactation put a childbearing women at particular risk of experiencing a loss of DHA. Animal studies indicate that decreased brain DHA in postpartum females leads to several depression-associated neurobiological changes that inhibits the brain’s ability to respond to stress appropriately. (13)
A 2014 study involving female fats found that menhaden fish oil benefits (which are rich in omega-3 fatty acids) include exerting beneficial effects on postpartum depression and decreasing the biomarkers related to depression, such as corticosterone and pro-inflammatory cytokines. (14)
A review published in the Journal of Midwifery and Women’s Health discusses the recent research on omega-3s and women’s mental health, with a particular focus on the perinatal period. These studies include population studies examining fish consumption and studies testing the efficacy of EPA and DHA as treatments for depression. The majority of studies indicate that EPA is able to treat depression either alone or in combination with DHA and/or antidepressant medications. (15)
Women who are pregnant are encouraged to get their omega-3 fatty acids, and other nutrients, from their food instead of supplements, so eating omega-3 foods such as salmon, walnuts, chia seeds, flaxseeds, natto and egg yolks during pregnancy can be helpful. For women with a history of depression, taking fish oil supplements in their last trimester and after giving birth may also be beneficial in fighting the symptoms of postpartum depression.
2. Acupuncture
Acupuncture is a holistic health technique that stems from Traditional Chinese Medicine practices in which trained practitioners stimulate specific points on the body by inserting thin needles into the skin. Many doctors are now recommending acupuncture as a treatment to reduce stress, balance hormones, and ease anxiety and pain during and after pregnancy. According to research conducted at Massachusetts General Hospital in 2012, acupuncture, including manual, electrical and laser-based, it is generally beneficial, well-tolerated and safe mono-therapy for depression. (16)
A study conducted at Stanford University in California analyzed the effectiveness of targeted acupuncture versus controls of a non-targeted acupuncture and massage in the treatment of women with postpartum depression. Eight weeks of an active acupuncture intervention targeted specifically for depression significantly outperformed a massage intervention by reducing depression symptoms that were measured on a rating scale. (17)
3. Exercise
According to the Journal of Midwifery and Women’s Health, there is now evidence to support the antidepressant effects of exercise for women with postpartum depression. Given the reluctance by some women to use antidepressant medication postpartum, and the limited availability of psychological therapies, exercise is a therapeutic and natural treatment for women who show signs of depression after giving birth. (18)
A 2008 study examined the effectiveness of an exercise support program on reducing depression symptoms childbirth. Eighteen women participated in the study, and they were allocated to either the intervention group (who received exercise support) or the control group (who received standard care) at 6 weeks postpartum. The exercise support consisted of 1 hour per week at the hospital and 2 sessions at home for 3 months. The study found that women who received the exercise support program were less likely to have high depression scores after childbirth compared with the control group. The researchers concluded that exercise benefited the women’s psychological well-being. (19)
4. Know the Signs and Plan Ahead
It’s important for new mothers to be aware of the signs and symptoms of postpartum depression, and to know that there is a possibility of developing this illness after giving birth. Pregnant women should attend classes or read about the risk factors associated with postpartum depression, such as prenatal depression, childcare stress, life stress and lack of support.
Communicating with your partner before giving birth can be helpful so that he/she is aware of your need for support, especially during the first months of infancy. It is even a good idea to plan in advance for help during the postpartum period in order to prevent fatigue, sleep deprivation and social isolation that can sometimes create vulnerability in postpartum women and make them more likely to develop depression. (20)
Closing Thoughts
- Postpartum depression affects up to 15 percent of mothers.
- Postpartum depression typically occurs within 4 weeks of giving birth and possibly as long as 30 weeks postpartum.
- The symptoms of postpartum depression include insomnia, crying spells, poor concentration, fatigue, mood swings and anxiety.
- Women who have a history of depression are most at risk for developing postpartum depression. Some other risk factors include a lack of support, marital dissatisfaction, childcare stress, life stress and prenatal depression.
- There is an adverse impact of postpartum depression on the infant, including issues with feeding, development and cognitive function.
- Conventional treatments for postpartum depression include psychotherapy, antidepressant medication and hormone therapy.
- Natural treatments for postpartum depression include omega-3 fatty acid supplementation, acupuncture, exercise and education.
- Knowing the risk factors and signs of postpartum depression before giving birth is important in helping new moms to prepare for the possibility of developing depression after childbirth.